

Comment to ACIP meeting of August 30, 2021 submitted by
Steve Kirsch - Executive Director of the COVID-19 Early Treatment Fund
stk@treatearly.org - September 1, 2021
NOTE:
This document is an updated version of the original August 29, 2021 US Government filing.
The most up-to-date PDF version is here.
ABOUT ME
I am the founder of the COVID-19 Early Treatment Fund (www.treatearly.org). Our work in funding early treatments for COVID was featured on 60 Minutes.
I am not anti-vax. I have been vaccinated and my entire family has been fully vaccinated as of March 30, 2021. I had fully bought into the narrative that the vaccines were safe and effective.Sunday, Sharyn Alfonsi reports on how a 40-year-old antidepressant became a possible candidate for early treatment of COVID. https://t.co/Q6Z8cuE5dr pic.twitter.com/rFf0INYRxR
— 60 Minutes (@60Minutes) March 5, 2021
Starting on May 9, 2021, I began to hear stories from my friends that were very troubling. For example, one friend had three relatives who were formerly healthy all die within days after getting the vaccine. Another friend had a heart attack 2 minutes after the injection and is now disabled, apparently for life. He’s 39 and has been told by his neurologist that the pain will get worse and worse every year. On a scale of 1 to 10, he’s a 10 every minute he’s awake. His life is ruined, likely forever, according to his doctors. That’s after just one shot.
I assembled a team of 20 doctors and scientists listed at the end of this comment to investigate the available evidence. The more we learned, the more concerned we got. When we tried to voice our concerns publicly, we were intimidated, censored, or ignored.
Nobody has responded with any evidence that addresses what we found and shows that we got it wrong.
Even more troubling is that nobody from the CDC or FDA would even respond to our repeated requests by email and phone to look at our analysis. They didn’t even want to see it.
All of this caused me to shift my position on these vaccines. I am against unsafe drugs, especially ones that disable or kill my friends.
OUR FINDINGS
Using the VAERS database and other official government data sources from the US and around the world (covering 35% of the world’s population), we found that the current vaccines are significantly more dangerous than has been previously believed.
Our most important findings include:
The “real world” fatality data from VAERS does not match the fatality data from the Phase 3 trials. They aren’t even close. Using multiple independent methods from independent researchers, we show that it is likely that over 150,000 Americans have already been killed (see Attachment 2). Even with a $1M reward to academics to spot an error in our analysis, there were no takers. It is urgent to resolve this discrepancy as soon as possible as we strongly believe that the real world data is right and the vaccines kill more people than they save. Even Pfizer’s own 6 month study failed to show any evidence of a net mortality benefit either before or after unblinding (at the end, 20 people who got the vaccine died vs. 14 people who got the placebo). And all three vaccines showed they significantly increase morbidity (highly statistically significant for all vaccines).
The vaccines should be stopped immediately based on the 150,000 Americans killed alone. Arguing about myocarditis cases and morbidity trade offs like they do at the ACIP meeting is like rearranging deck chairs on the Titanic. We have never had a vaccine in recent history that has killed 150,000 Americans. The H1N1 vaccine was stopped in 1976 after killing around 32 people. Today, we ignore all these deaths, writing them all off to “bad luck.”
None of the COVID vaccines reduce all-cause morbidity. It’s the opposite: they all significantly increase all-cause morbidity by as much as 4.2 times baseline (p<=0.00001). The CDC must know this since this information is hiding in plain sight in the published literature. What is the point of offering an optional medical intervention which significantly increases all-cause morbidity when safer alternatives such as early treatment are available?
There is an error in the adverse event detection formula used by the CDC that appears to have prevented the CDC from seeing the safety signals that were obvious to our VAERS experts.
Early treatment and prophylaxis protocols are a superior option to the current vaccines on every single meaningful metric:
Higher relative risk reduction (over 99%)
Simple prophylaxis protocols be used to prevent infection with up to 100% success without the use of any drugs whatsoever
Greater safety (minor temporary side effects, known safety profile)
They lower both all-cause mortality and all-cause morbidity
They work equally well on all variants
They do not promote escape variants
They do not cause vaccine enhanced infectivity/replication
They do not cause prion diseases
They prevent long-haul COVID syndrome nearly 100% of the time
They enable people to acquire recovered immunity which is both 13 times stronger and more durable than vaccine-induced immunity (this story says it is 27 times better)
Because of all of these advantages, all early treatment methods are being deliberately sabotaged by the FDA and NIH so that people will believe that the vaccines are the only option. Even when drugs are proven in high quality large Phase 3 trials (fluvoxamine), or when there are multiple systematic reviews showing ivermectin is an effective early treatment for COVID (Lawrie ivermectin systematic review showing 62% reduced mortality and Zein ivermectin systematic review showing 61% reduced mortality), the NIH and medical community ignores these treatments and rates them as NEUTRAL which doctors all take as a sign to avoid. Most pharmacies will not fill ivermectin prescriptions anymore (they did this AFTER both ivermectin systematic reviews were published which is a new low for evidence-based medicine). Some pharmacies will report physicians to the medical boards who prescribe ivermectin. You can get ivermectin on Amazon, but the wait is months. Amazon conveniently puts a notice on the web page that The FDA advises against the use of ivermectin to treat or prevent COVID-19 but does not inform consumers of the peer-reviewed systematic review and meta-analysis. The ACTIV-6 trial deliberately underdoses ivermectin (with just 3 days of treatment at a lower than effective dose) so it will fail to have an effect so they can “prove” to the world they were right. This is a waste of taxpayer money because everyone will concede that the trial they are running will fail. Watch this CNN video where Dr. Lena Wen conveniently references the systematic review that she claims “proves” ivermectin does nothing (it limited the studies it looked at and found that ivermectin reduced mortality by 60%, not 0%) and she claims that one of the safest drugs ever invented is risky, and she conveniently ignores the higher quality systematic review that shows that ivermectin works (that one gets no mention). The FDA made NAC available by prescription after it was proven to work for COVID even though there have never been any deaths from NAC in 60 years and it is incorporated into 1,100 different products all of which had to be reformulated. What was the reason for that? They pull a drug that kills no one, and approve a vaccine that kills 2 people for every 1 it saves and make it available without a prescription.
Nobody of any stature in the medical world will agree to publicly debate our team on any of the issues raised in this document, even with huge financial incentives to do so. People at the NIH, FDA, and CDC refuse to comment or respond to any of the issues raised in this document. Dr. Lena Wen, Eric Topol, Monica Gandhi, etc. will never debate us because they will be discredited. You never see fair and balanced coverage. CNN only has qualified experts on one side of the issue; they never hear from anyone competent who will provide a balanced view for the public. This CNN video is typical: all three talking heads are bashing early treatment.
The censorship and intimidation done by doctors, the White House, mainstream media, and social media companies makes it so everyone is afraid to speak the truth is unprecedented. Censorship is used on all social media platforms to keep this information out of public view. Reporters who attempt to write stories find that they will not be published. Fact checkers will not reply to corrections on their fact checks. Top academic scientists who seek to challenge the narrative with peer-reviewed papers find that the papers never make it into the journal. When we pointed out Phase 3 clinical trial fraud (Maddie de Garay), the FDA promised to investigate and did nothing. This is not how science is supposed to work but no one in the mainstream academic community (except for Peter Doshi of the BMJ and even he has to be very careful) is speaking out about this.
In Congress, Senator Ron Johnson has been the only member to speak out about what has happened. Everyone else in Congress is afraid of being labelled “anti-science” if they oppose the vaccines. Nobody in Congress (except for Johnson’s staff) will talk to me after one meeting because they can’t answer any of my questions like “How many people have to die before you will call for a halt to the vaccination program?” or “Why aren’t you asking the NIH for Fauci’s unredacted emails?” or “How do you explain how Dr. Peter Schirmacher one of the world’s top pathologists finds 30% to 40% death rate after vaccination while the CDC hasn’t found any deaths?” These are the questions that the press should be asking, but aren’t. Investigative journalism is dead. The media is simply amplifying the false narrative of the White House and ignoring the science.
Experts like Dr. Geert Vanden Bossche, Dr. Robert Malone, Dr. Peter McCullough, and others have been right about these issues since they started speaking out, but they are being ignored or censored by the mainstream media.
It is insulting to us for the ACIP committee to ask for comments before the meeting and then vote on approving the vaccine before reading any of the comments. The ACIP committee is sending a very clear message to the public that any comments made will be ignored. The public comment process is for show. This is doubly insulting to me personally as I tried to directly contact ACIP members and they all said file it as a public comment. Did that. It never gets read.
We recommend the committee take the following actions:
Require autopsies for all deaths within 4 weeks of any COVID19 vaccination so that data is available to compute an estimate of the true all-cause mortality.
Make available the analysis of the 11,000 deaths investigation in VAERS for public inspection. It’s important for the public to understand why the CDC couldn’t attribute a single death to the vaccine whereas one of the world’s top pathologists ascribed at least 30% of all deaths to the vaccine.
Explain publicly why there is a death peak on the second day after vaccination if the vaccinations are perfectly safe and not causing deaths.
Explain publicly why the severe adverse side effects are dose dependent
Publish the proper elevated event table (see Attachment 2. Page 17)
Publish your analysis of the VAERS data including the propensity to report factor and the under reporting factor for fatalities or serious events. Please show us the correct analysis showing that there are no excess deaths this year as has been claimed.
Meet with our team as soon as possible to assess the validity of the points above.
Fix the adverse event signal detection system so it can at least recognize all the serious adverse events identified in Attachment 2, page 17.
Review the VAERS multiplier used in the myocarditis analysis. It appears to be 1. That makes absolutely no sense to us. How was that justified?
Recommend that vaccine mandates should not be issued without evidence of a statistically significant all-cause morbidity decrease (which there is not in this case).
Define a COVID vaccine stopping condition after which that vaccine should be halted until the stopping issues are addressed. In 1976, the stopping threshold was 32 deaths.
Ask the CDC to engage with us in a public discussion on vaccination issues so the public can hear first hand from qualified experts on both sides. This is a more effective way to combat vaccine hesitancy than censorship.
If the meetings with our team result in the validation of our assertions, then the following actions should be considered:
Recommend that at least three classes of people should not be vaccinated and should use early treatment if infected:
Previously infected
Women who are pregnant or might soon become pregnant
Anyone under age 50
Inform the public of the complete list of elevated risks and their rates for the COVID vaccines.
THE MECHANISM OF ACTION OF THE COVID VACCINES IS DIFFERENT FROM THAT OF TRADITIONAL VACCINES
Dr. Robert Malone has described the vaccine as causing a cytotoxic spike protein to be produced throughout the body for up to 48 hours, with the potential to cause blood clots, inflammation, and permanent scarring. In addition, the spike protein (particularly the S1 segment) could break free of the cell and freely circulate, causing damage which could lead to a very wide range of pulmonary, cardiovascular, and neurological events.
The gene-based vaccines (i.e., the 3 vaccines used in the US today) work in a completely different way than classical vaccines. With the latter, a fixed dose of killed or weakened pathogen or a toxin from the pathogen is injected and this sets a precise upper limit on how much foreign material is administered. In the former, while a fixed dose is also given, the upper limit of how much antigen is expressed depends on a series of steps each with substantial variability. This unavoidably greatly widens the range of amounts and concentrations of toxic spike protein in the body. Compounding this is the variability in anatomical distribution of the product with some body parts more prone to injury than others.
This built-in variability means that gene-based vaccines will likely always be much less safe than a classical vaccine. While the majority of people have no serious adverse events whatsoever, a significant number of people, perhaps in the millions, can be profoundly affected with one or more of a wide range of serious symptoms. Females are nearly 2.5 times as likely to be affected as males.
In particular, the VAERS data shows these symptoms include brain hemorrhages, strokes, heart attacks, multiple organ failure, pulmonary embolisms, and even sudden unexpected death.
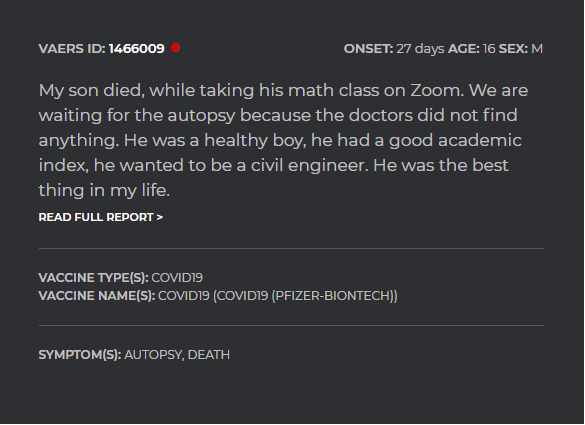
A person can be perfectly normal and then just drop dead unexpectedly as the ACIP team already knows through their recent examination of the VAERS records of children 12-17 who died. For example, a 16 year old California student died unexpectedly in the middle of a Zoom math class. He had no prior health problems and appeared completely normal 20 minutes before his death.
If he didn’t die from the vaccine, what did he die from?
There is a partial list of the elevated symptoms identified by VAERS analysis in Attachment 2, page 17.
Nearly every cardiovascular and neurological event occurred at a rate that was 10X or more than would be expected to be reported in a typical year by all of the vaccines in that year.
IT IS VITALLY IMPORTANT THAT ALL PHYSICIANS BE EDUCATED ON BOTH THE MECHANISM OF ACTION OF THE VACCINE AND THE RANGE OF SYMPTOMS THAT ARE BEING CAUSED ASAP BECAUSE IT IS COMPROMISING PATIENT CARE
Today, most doctors believe the vaccines are completely safe. There is virtually no knowledge of vaccine symptoms. This causes physicians to treat these symptoms as if they are caused by something other than the vaccine which results in treatments that are ineffective since they are not treating the underlying cause.
Maddie de Garay is a perfect example of this. She will pay the price of preventable misdiagnosis for the rest of her life because physicians were never informed that the vaccines could be causal for her symptoms; the doctors treated Maddie as if symptoms were all in her head.
Angela Wulbrecht who has been a nurse for 23 years in Northern California is another example. She was misdiagnosed by the world’s best experts because the CDC never disclosed to anyone that the vaccines are super dangerous and how the vaccines can disable or kill people. She only found relief when she consulted Dr. Bruce Patterson who understood that the vaccines are deadly. She was able to get relief from her symptoms only when she was given drugs that targeted the vaccine damage.
Both of these people are public figures and are willing to speak out if you want to talk to them.
THE PROPER SAFETY TESTS WERE NEVER DONE
The FDA made the mistake of regulating the three COVID vaccines as a vaccine exclusively. As a result, the dose, duration, and amount of spike protein produced by these vaccines were never measured in advance of approval by the FDA.
Today, despite the evidence of unforeseen and unprecedented harm, these three critical parameters are still completely unknown.
Why haven’t these tests been done in non-human primates with the actual vaccine?
THE D-DIMER AND CRP BIOMARKERS ARE A SMOKING GUN THAT THESE VACCINES ARE NOT SAFE
Even more concerning is that there has been no attempt to measure biomarkers that could clearly show that these vaccines are causing unexpected harm.
For example, measuring C-Reactive Protein and D-dimer of people before and after vaccination is a very simple experiment to show that the vaccines are causing problems.
Multiple researchers (contact us for the details) have done such a study in hundreds of patients and found that both biomarkers are elevated above normal levels for around three months in over 60% of patients.
This is very serious. It is a smoking gun that indicates that something is very wrong with these vaccines. For example, a 73 year-old female on her second dose had a D-dimer of 1186 ng/mL (normally it is less than 250 ng/mL) two weeks after the shot. It remained above normal for three months.
AN OVER-RELIANCE ON DELEGATED TRUST HAS MAGNIFIED SMALL ERRORS INTO LARGER ERRORS
We live in a world of delegated trust. But if the root of that trust makes a mistake, it creates a ripple effect where the consequences are magnified exponentially.
Our first example of amplified errors due to delegated trust is the safety signal detection of the VAERS database that John Su at the CDC has been monitoring.
The ACIP committee trusts the CDC staff to monitor VAERS. If there is a bug in the monitoring algorithm used by the CDC, the CDC will miss the critical safety signals and the ACIP committee will not be alerted. ACIP members do not have the time or expertise to analyze the VAERS data themselves, as it is not a simple task, requiring many months of dedicated effort using specialized tools. If such a critical safety signal is missed by the CDC, there are immeasurable consequences and harm to the public.
When we looked at the VAERS database, we found dozens of very serious safety signals that the CDC failed to detect.
The attached analysis (see Attachment 2, page 17) shows that every neurological and cardiovascular event that we investigated was strongly elevated as compared to previous vaccines, most by at least 10X and some by as much as 473 times higher than what is normally expected in a typical year across all vaccines. This is impossible to explain if the COVID vaccines are perfectly safe.
We just received a similar analysis from Professor Josh Guetzkow which can be viewed at Attachment 3. In Table 1, for example, death is happening at a rate 91X higher than normal. That sort of increase cannot possibly be explained by “stimulated reporting” or “more people got vaccinations.”
This is independent confirmation that the explanation from the CDC and FDA does not match reality. The ACIP committee is also clueless about this and apparently lacks basic critical thinking skills.
All the evidence has been in plain sight since January 2021, not just in VAERS, but to those practicing doctors, neurologists, and pathologists who were seeing a huge spike in adverse events and deaths and were willing to consider the possibility that the vaccines were not as safe as had been claimed by the CDC and FDA.
In addition, all of the neurological and cardiovascular symptoms with elevated event counts were consistent with the mechanism of action described at the start of this comment. Each and every symptom we looked at satisfies all the traditional Bradford-Hill causality criteria using both absolute rate elevation compared to baseline rates as well as Dose 1 vs. Dose 2 response disparities.
A BUG IN THE SAFETY SIGNAL ALGORITHM ALLOWS SAFETY SIGNALS TO ESCAPE DETECTION
Why was the CDC oblivious to these same signals? The answer: a bug in the algorithm used by the CDC. This bug only manifests itself when the vaccine being monitored produces a wider than normal range of side effects. This has not been the case with earlier vaccines which is why it wasn’t detected earlier.
The bug in the safety signal algorithm is documented in this post: https://roundingtheearth.substack.com/p/defining-away-vaccine-safety-signals-572 (this is Part III, which contains links to Parts I and II). We would be happy to meet with CDC staff to go over this in detail.
WHY ARE YOU IGNORING PEOPLE WHO ARE TRYING TO HELP YOU SPOT SAFETY SIGNALS?
Repeated attempts to inform any ACIP committee member of this anomaly were unsuccessful.
Considering that the ACIP committee is tasked with the critical monitoring of safety in the world’s single most important drug, we are puzzled by the lack of interest in receiving safety information from qualified researchers. We were directed to submit comments to a non-existent docket number.
Failing to get anyone on the ACIP committee to respond, we next attempted to communicate the signal error to the CBER group at the FDA. Not one person responded, including Dr. Steven A. Anderson and his staff, despite multiple emails and phone calls. Again, we are puzzled by the lack of interest in receiving safety information from qualified researchers. Dr. Anderson had said in a video call that he was the main person responsible for the safety monitoring.
Emails to both John Su and Anne M. Hause were also not responded to.
Perhaps the FDA and CDC should simply let people know that “if you find an urgent safety problem, don’t bother to contact us because we aren’t interested in hearing what you have to say.”
If this were more well known, it would have saved our time and yours.
MYTH BUSTED: “VAERS CANNOT BE USED TO SHOW CAUSALITY”
For the current COVID vaccines, our team is extremely confident that we can meet all the Bradford-Hill criteria for causality using VAERS analysis alone. Will our statisticians and VAERS experts be permitted to meet with any ACIP members to discuss the data?
For example, it is well established that a clear dose dependency relationship can be used to satisfy one of the Bradford-Hill criteria. Because two of the vaccines are multi-dose vaccines, a Dose 1/Dose 2 ratio analysis shows a very clear signal. Sadly, this type of analysis is currently being completely ignored by the CDC.
THE FDA HAS ASSUMED THAT VAERS WAS JUST OVER-REPORTED THIS YEAR
Our second example of amplified errors due to delegated trust is the calculation of the VAERS event counts.
A detailed analysis of the VAERS data (Attachment 2 and Attachment 3) both show that the FDA has made a very serious error in assuming (without any evidence whatsoever as far as we’ve seen) that the propensity to report to VAERS is much higher this year and that these are simply all background events that can safely be ignored. The two analyses found the same thing and were done by different people, in different countries, who never met. The results were the same.
The problem with the FDA assumption is that their hypothesis simply doesn’t fit the data. If it was simply reporting background information, we’d see only a slight bump on the first day, and each day would get progressively smaller. That’s what we’ve seen for all vaccines for the past 30 years. But this one is shaped completely differently (see the attachments for details).
If the propensity to report is drastically increased, then it should be easy to prove us wrong. Randomly survey 100 neurologists and ask them the number of reportable events vs. reports filed last year vs. this year.
One of the nation’s top neurologists (she’s listed in US News & World Report) told us she had significant events for 2,000 patients that should have been reported in VAERS and got so frustrated with the time commitment after making just 2 VAERS reports she stopped doing it. Note that she believed she was NOT required by law to report it, only the person who did the vaccination is. So she reported just 1 in 1,000 events. I asked her how many VAERS reports she’s posted in the past. She said zero. I asked her why. She said, “Because there was nothing to report.”
Dr. Bradley Campell started looking at the bloodwork of his patients pre- and post-jab. Watch this video at 35:30 where he describes a patient whose troponin levels were 26 times normal after the jab. Was this a fluke?
A physician in Canada said he’s only made only 1 vaccine report to the Canadian healthcare system in the last 29 years. This year he’s filed 25 so far. At first they rejected them, but now they are accepting them all.
Other anecdotes we’ve heard many times from patients is when doctor A talks to doctor B and it goes something like this: Q: “Did you report it to VAERS?” A: “Of course not!”
Most consumers don’t know anything about VAERS.
The actual reason VAERS is over-reported this year is because there are so many events to report, a possibility that the FDA never considered.
We are waiting to see the evidence from people claiming that it is overreported. So far, all the evidence and anecdotes we do have shows it isn’t. The VAERS data, properly analyzed, show no over reporting, and the physician surveys we’ve done show no evidence.
The FDA continues to stonewall with their evidence supporting their claims. We’ve seen nothing from the FDA after months of asking that supports their point. No data. Nothing. Why not just show us the evidence
THE CDC CLAIMS “ANYONE CAN REPORT TO VAERS”
Many people assume that the large number of VAERS reports are due to anti-vaxxers gaming the system. But none of them can provide any evidence whatsoever that that is true. It is a claim that fits the narrative that is done without looking at the data at all. There is no such analysis.
In fact, when you do the analysis of the data, you find that 86% of the reports are consistent with vaccine injury and the other 14% lack enough information in the reports to tell. See the Mclachlan study.
So the evidence shows the opposite. If you make the claim the reports are all fraudulent, you need to show the analysis to back up the claim.
Interestingly, the people who make such claims on no evidence are the same people who demand peer-reviewed research to believe OUR arguments.
It is a federal offense to file a false VAERS report and all reports are screened by HHS (including requesting the medical records) before being published.
We are aware of 2 false VAERS reports in over 1.4M records. So it is true that not everything in VAERS is true, but the number of false reports is small and both of the reporters were referred to the FDA for prosecution.
YOU CAN LEARN A LOT BY TALKING TO A NEUROLOGIST
Some of the things we learned by talking to a neurologist with over 15 years of experience and a 20,000 patient practice are worth keeping in mind:
They can’t reveal their identity publicly or they would lose their license
They can’t speak out against the vaccine to their patients or risk loss of license
Patient load went up 20X during the vaccine rollout. Never saw anything like it in her career.
Over 2,000 patients had serious side effects from the vaccine
They only reported 2 to VAERS: it was too frustrating to use; it would crash every 2 minutes and you’d have to start over from scratch.
Only the doctor doing the injection must report to VAERS, so they don’t have to, so they stopped doing it since it was so cumbersome.
Has always known about VAERS, but never need to use it before since never had to report an adverse event!!! This year would have reported all 2,000 patients if VAERS was easier to use. Instead, made just 2 reports (1 of 1,000)
Neurologists are now booked up for 3-4 months is typical. At Stanford is 6 months.
Most neurologists are clueless on how to treat vax events. Most neurologists don’t associate the vax as the cause of the problem. Treatments are useless. When patient goes on Patterson treatment protocol, they can recover back to “normal” in 8 weeks. However, they get no medical training at all on this (because doing so would be an admission that the vaccines aren’t safe) so most people who are vaccine injured remain disabled.
At UC Davis, 40% of staff is unvaxed. They have to wait in line twice a week and come in 2.5 hours early to get in line for COVID testing. They endure that because they’ve seen first hand how bad the vax reactions can be.
Long-term impact of the vaccination program: Increase in multiple neurological conditions.
For the vaccine injured, the standard blood tests (including all extended testing such as CRP, D-dimer, etc) can all show completely normal. Angela Wulbrecht was given every test under the sun and they were all normal. It was only when she took Patterson’s cytokine panel and S-protein tests that showed she was clearly very sick.
FDA FALSE STATEMENT: “DEATHS CAUSED BY THE VACCINE ARE EXTREMELY RARE”
In a letter dated August 23, 2021, Janet Woodcock writes to Senator Johnson, “Reports of death after COVID-19 vaccination that are found to be related, or even possibly related, to vaccination with COVID-19 vaccines have been extremely rare.”
Where are the 249 autopsies on which that statement was made? Has the committee reviewed all 249 autopsy reports?
We were able to prove causality using the Bradford-Hill criteria from just the VAERS data alone. We didn’t need the autopsies.
It was shocking to us that the CDC and FDA couldn’t find these signals despite access to 249 autopsy reports.
There is something seriously wrong here. You cannot have a few excess deaths from the vaccine when both the VAERS database itself and the data from other countries shows that there have to be 150,000 deaths. They both cannot be right. We think the CDC is mistaken because the death data we used to compute the 150,000 deaths comes from 35% of the world’s population. This error needs to be corrected as soon as possible.
SYMPTOM CODE FOR A VACCINE DEATH
What is the SYMPTOM code for a vaccine death? We looked at all the VAERS records with autopsies and we couldn’t find a single record with a coding for a COVID VACCINE DEATH.
OUR ANALYSIS SHOWS THAT IT IS HIGHLY LIKELY THAT OVER 150,000 PREVIOUSLY HEALTHY AMERICANS HAVE BEEN KILLED BY THE COVID VACCINES IN 2021
The analysis in Attachment 2 shows that 150,000 previously healthy vaccinated Americans have had their lives cut short prematurely due to the vaccines. We confirmed this number using independent methods from independent researchers. We used both US data and data from other countries. Our analysis used data from over 35% of the world’s population.
Our results are also consistent with reports from doctors we know who report that they have lost more patients to the vaccine than to COVID. For example, one doctor with 700 patients lost 2 patients to the vaccine and no patients to COVID. These doctors are special because they are “vaccine aware” and understand the mechanisms of action. In another case, one nursing home with 132 beds lost two patients within hours after vaccination.
Unfortunately, most doctors are blind to the association between the COVID vaccines and deaths and if asked, always report 0 vaccine deaths because they believe the narrative that the vaccines are “safe and effective.” Any deaths would be anecdotes and ascribed to some other cause. For example, when the fetus of a recently vaccinated pregnant woman had a massive brain hemorrhage, the doctor considered the event caused by a “genetic defect.” The vaccine is never even considered as a possible cause.
As far as we know, not a single doctor in the US has determined that any deaths were caused by the COVID vaccines. There isn’t even a column in the CDC weekly report for deaths from the COVID vaccine. Apparently, it is impossible to die from the COVID vaccines if you live in the US.
However, a methodology based on excess death analysis (as detailed in Attachment 2) and autopsy results in other countries of people who died after getting the vaccine tells a completely different story: a story of a very deadly vaccine that has likely killed over 150,000 Americans so far.
It has been enormously frustrating to us that the CDC and FDA look the other way and have ignored all our attempts to share our analysis. That is not a good safety practice to ignore qualified people who disagree with you, especially when 150,000 lives are at stake. This is not serving the public interest. Safety must be a top priority at these agencies but when there are deaths from the vaccine, people are simply looking the other way and don’t want to hear it. This is why all our attempts to contact people were ignored.
If the CDC or FDA engages with us and finds an error in our analysis and can show evidence that no lives have been lost to the vaccine, then this would do wonders for reducing vaccine hesitancy. Conversely, if the CDC or FDA confirms we are correct, we can immediately stop future loss of life by aborting the vaccination campaign.
Whichever way it ends up, the clarity that happens when both sides engage in an open public discussion of the methods and evidence used will benefit all parties and the public.
THERE IS NO EVIDENCE ANYWHERE OF AN ALL-CAUSE MORBIDITY BENEFIT. WITHOUT THAT, DEPLOYING THESE VACCINES MAKES NO SENSE, ESPECIALLY SINCE SUPERIOR ALTERNATIVES ARE AVAILABLE
When a vaccine class is generating a huge number of adverse events in 8 months that are more than the events from all 70 vaccines over the past 30 years, it is reasonable to assume that there might be a significant safety problem with the vaccine.
In such a case, rather than focusing on the reduction of relative and absolute risk provided by the vaccine, it is instead more important to focus on whether there is a significant reduction in all-cause morbidity.
For the three vaccines, using data from the original clinical trials, it has been shown that in all cases, the all-cause morbidity is significantly elevated by all the vaccines. The elevation ranges from 1.5X to 4.2X. That is a large move in the wrong direction. It is highly statistically significant for all three vaccines. This of course is consistent with what we find in VAERS.
With respect to efficacy, nobody argues that the vaccines have saved people from dying from COVID. But the problem is that this benefit comes at a steep cost: an increase in death from other causes that completely negates the benefit of the reduction in COVID-related deaths.
But could an all-cause mortality benefit compensate for the higher all-cause morbidity? Our best data on that is the Pfizer 6-month study. A 50% reduction in COVID deaths was more than offset by a four times higher rate of cardiac arrest. As a result, the all cause mortality rate was higher in the treatment group than in the placebo group. This was true in both the pre-unblinding and post-unblinding phases. The numbers were small but the point is that there is no demonstrable all-cause mortality benefit. Zero. If anything it was the other way around.
As evidenced by the high number of severe adverse events reported to the VAERS system, it is the all-cause morbidity statistic that is the new elephant in the room. If you can’t show a lower all-cause morbidity, there is no reason to vaccinate.
For the three vaccines, using data from the original clinical trials, it has been shown in the peer-reviewed literature that in all cases, the all-cause morbidity is significantly elevated. The elevation ranges from 1.5X to 4.2X. That is a large move in the wrong direction. It is highly statistically significant for all three vaccines. This of course is consistent with what we find in VAERS.
THE VACCINES KILL MORE PEOPLE THAN THEY SAVE (3 INDEPENDENT SOURCES)
We also have troubling anecdotes like the nursing home with 136 beds where all the residents were given the booster just before September 1 and now 4 of them are dead and 7 hospitalized as a result. We are keeping the nursing home secret for now to protect our whistleblower.
This is a 3% death rate from the vaccine. We only found out about this through an insider. The media never covers this because they don’t want to panic the public reporting on an anecdote that would dissuade people from taking the safe and effective vaccine.
Let’s compare this to the expected COVID deaths (without a vaccine). Using 156 deaths per million in US for 65+, we’d expect to see 1 COVID death per year among that population of 136 (assuming all the beds were filled). But the rates might be higher for nursing homes, but the rates of COVID are lower today due to all the vaccinations so that’s probably a wash.
So if the vaccines remain 100% effective for an entire year, over a 1 year period we are killing 4 elderly per COVID case saved. This is not a good tradeoff.
But it’s even worse: 7 people got hospitalized. Some of those may die shortly or have their lives cut short.
Thanks to a courageous whistleblower Abrien Aguirre we can confirm the death toll from the nursing home. Aguirre said that they had 32 vaccine deaths vs. 16 virus deaths. In other words, the vaccine has killed twice as many people as the virus in the very setting that the vaccine is supposed to be the most beneficial.
So in both cases, the vaccine is killing more people than COVID (4:1 and 2:1).
This is why all the nursing homes keep all this information secret so the public never knows about it. Each nursing home thinks they are simply an unfortunate anecdote, where the reality is that their numbers are normal for this vaccine. If you try to call the homes directly, they won’t talk. Nobody returns your calls. So nobody ever finds out.
What makes those two anecdotes interesting is that the whistleblowers understand how the vaccines kill. Most other nursing homes don’t make the connection and will tell you that no one has died from the vaccine (they’d just say they died from natural causes).
Since the vaccine can also kill you over a 3 month period, they simply assume that the patient died from natural causes (like a massive heart attack or just “died”) and it just “happened” that a lot of deaths coincidentally happened around vaccination time, but nobody is doing the statistical calculation.
And since most nursing homes are small, a 3% death rate looks like “natural causes.”
Was he lying? What was his motivation? Aguirre basically put all his income on the line. For what? His reward: Aguirre was fired for telling the truth. This is exactly why people at nursing homes will not say anything. Here is the follow-up video.
There is only punishment if you tell the truth. This is why the nursing home whistleblower isn’t identifying himself/herself.
Neither nursing homes would talk about the correct data. Why wouldn’t they correct the data if it is wrong? Why are they hiding in the shadows?
But you don’t have to believe these anecdotes. Another story just came out based on UK data:

And another commenter to ACIP had similar numbers using yet another approach.
So if you have different data that shows the opposite, we’d love to see it! So we have three independent sources now showing the vaccines are deadlier than the virus.
NOBODY WANTS TO TALK ON THE RECORD FOR FEAR OF LOSING THEIR JOB
One of my vaccine injured friends said the head anaesthesiologist at one of the world’s top medical schools said “he wasn’t willing to put it in writing” that it was caused by the vaccine because it would affect his reputation. However, his medical assistant was willing to put it in writing and sacrifice her career. My friend was told his symptoms would get worse over time. He’s 39 years old and his life was ruined by the vaccine and nobody wants to end their career to speak out.
One of the top neurologists in my area (over 20,000 patients) won’t talk publicly.
I talked to a medical examiner who didn’t even feel comfortable sharing her name with me, but revealed autopsies are useless.
Basically everyone who could talk won’t. They can’t speak out publicly or they will lose their license.
They could speak to a reporter and talk without their names being disclosed, but no mainstream media would run the story, so there is no point. Reporters at top newspapers cannot get their stories run. 60 Minutes won’t touch the story either.
MEDICAL EXAMINER SAYS AUTOPSIES ARE USELESS, VAERS IS THE GOLD STANDARD FOR CAUSALITY
We were only able to find one medical examiner who would talk to us. Even then, she wouldn’t reveal her last name or state.
Here are the key points:
She is the only ME in her state looking at vaccine-related deaths. The other ME’s all assume the vaccines are safe so never will implicate the vaccine.
The ME’s in general don't have the skills, they don't have the proper tests to determine causality for deaths caused by this vaccine (they don’t exist in the post-mortem setting), they don't have the time, they don't have the medical records, and they get the body too late. They can see large blood clots of course
THEY CAN'T EVEN ORDER A D-DIMER because they are told "well that's not generally done" so unless they fight for it, they simply give up.
They even get a huge push back when asking for the medical records.
Often, they don't even know the vax status or when the patient was vaccinated.
She had to personally make a call to the family to determine whether a patient got vaccinated.
THIS IS WHY the ME’s cannot make the connection in the autopsy setting.
She trusts VAERS way more than autopsy....says **NOBODY** is going to find this post-mortem
She never had time to report any of her deaths in VAERS.... the ME's are overloaded with some cases from 6 months ago still not completed.
She was operating today on 3 hours sleep. They are understaffed and overworked. It’s exhausting.
For vax deaths, she said autopsies are NOT the gold standard. It is VAERS.
CALCULATION OF REDUCED LIFESPAN
It is difficult to make a tradeoff between the elevated morbidity that reduces lifespan and the number of COVID deaths saved.
The COVID vaccines introduce both morbidity and mortality risks.
What ACIP has done is compare morbidity due to the vaccine vs. the same morbidity from COVID. That can be problematic if some some morbidities are improved and some are made worse. We’d have to look at all morbidities, something that ACIP hasn’t done since they haven’t seen the safety signals.
We believe that if we just look at the increased mortality due to the 1) direct deaths caused by the vaccine and 2) the reduction in total lifespan from all serious adverse events elevated by the vaccine, it would be clear that there is no mortality benefit.
We can see that from the Pfizer Phase 3 6 month study where more people in the treatment group died both pre- and post-unblinding. The Hawaii nursing home data is consistent: there was a 2:1 vaccine caused death:max possible vaccine saved death ratio which also supports stopping the vaccine.
Therefore, it seems likely to us that not only is there no morbidity benefit from the vaccines, but there is no all-cause mortality benefit from the vaccines either.
This makes the vaccines very hard to justify.
If we are wrong, we’d like to see the analysis.
WE ESTIMATE THAT APPROXIMATELY 574 KIDS HAVE BEEN KILLED BY THE VACCINE SO FAR; THAT’S MORE THAN HAVE DIED FROM COVID. WE ARE MAKING A HUGE MISTAKE. WE ARE KILLING OUR KIDS, NOT SAVING THEM.
The ACIP committee recently analyzed the cause of death of the 14 kids (aged 12 to 17) whose fatalities were recorded in the VAERS system. Had they had the table in the attached document, they would have realized that in every case (where there was sufficient symptom detail), the main cause of death was consistent with a symptom that was strongly elevated by the COVID19 vaccines. This should have led to a different outcome Mortality Among Teenagers Aged 12-19 Years: United States, 1999-2006 than simply listing the causes of death of the kids with no further discussion. No concern over the lack of autopsies was noted in the meeting notes. It is very likely that none of the kids had an autopsy done. There was no mention of this in the report.
We believe the lack of autopsies is a huge oversight for a vaccine that is generating so many legitimate adverse events. We believe it is imperative for the ACIP committee to immediately demand that autopsies be done. How many more kids must die before we look to find the real cause of death?
These children are dead now and their lives can never be recovered. But we can learn from their death if the ACIP committee members would simply read the 14 VAERS reports on each child and compare the cause of death with the symptoms listed in the table in the attached paper.
Five kids dying from cardiac arrest is not normal. Kids between 12 and 17 are twice as likely to die from cancer (6%) as from heart disease (3%). In this case, 38% died from heart disease and 0% died from cancer. That’s statistically very unlikely. It points to the undeniable fact that these kids did not die of natural causes. Therefore, the hypothesis that the vaccines are safe seems highly unlikely. How does the ACIP panel explain this?
One of the children died with an intracranial hemorrhage. How could that have not raised a huge red flag. Kids that age never die from an intracranial hemorrhage.
We did a search in VAERS searching every record, over 70 vaccines over the last 30 years. There were only two deaths of kids aged 12-17 with “HAEMORRHAGE INTRACRANIAL” in the history of VAERS and both were associated with the recently approved Pfizer vaccine. There weren’t any deaths caused by an intracranial hemorrhage in the entire history of VAERS in that age range until the COVID vaccines arrived on the scene. One event could be written off as a fluke--- very bad luck. But two events are a complete train wreck. How this didn’t raise any red flags in the ACIP committee is a mystery to us.
As this note is being written the BBC News just reported that BBC presenter Lisa Shaw died of a brain haemorrhage. The coroner determined the cause was the COVID vaccine. All of the causal factors in her death were consistent with the elevated symptoms we found in VAERS. Note that the Astra-Zeneca vaccine has a nearly identical mechanism of action as the mRNA vaccines.
Each of the 14 children who died in the CDC study represents 41*14=574 real deaths (as noted in the attached paper). Thus, more American kids have already been killed by the COVID vaccines than have been killed in the entire history of COVID to date (361). That’s tragic.
Two of the kids died from a pulmonary embolism, a symptom that is very strongly caused by the vaccines. Over 5 years in VAERS, you’ll find just one PE death in that age range. So to get one PE death in a year, that’s bad luck. To get two, you have to at least say that it’s more likely than not that it wasn’t just random. Yet the CDC report dismissed it without comment.
AN ACCURATE MYOCARDITIS COST-BENEFIT ANALYSIS IS MISSING
The CDC myocarditis cost-benefit analysis omitted the determination of the VAERS under-reporting factor for “mild” events.
While we think myocarditis is a serious event, the CDC characterizes these events as “mild” and thus would be less likely to be reported than something “severe” like death.
Therefore, we’d estimate that the VAERS under-reporting of such an event might be somewhere around a factor of 100.
My question to the panel is whether a 100 times greater rate than the rate reported in the report would make a difference in the recommendation of the ACIP panel? We would be very surprised if this doesn’t change the recommendation.
Also, as a sanity check on our results, please refer to Table 1 in Attachment3 which is Joshua Guetzkow’s analysis showing a 91-fold increase over baseline myocarditis rates.
Also, it would be good to estimate the effect of this heart damage (and all other conditions elevated by the vaccines) on expected lifespan so it is clear that the shortened lifespan is worth the savings in the amount of deaths. This way, we can do a pure mortality tradeoff.
For a lot of AEs, the quality adjusted life years (QALYs) is not significant. For young people, myocarditis represents an enormous QALY calculation. This will include some deaths, but most of a lifetime of a large range of reduction of life value.
For public health officials to discard the data without acknowledging something like a QALY comparison (and the deaths) is inappropriate.
TRUSTING THE PHASE 3 TRIAL RESULTS AS THE “GOLD STANDARD” IS NOT A GOOD IDEA
When there is a disagreement between real-world results and the Phase 3 clinical trial, we think it is better to trust reality. Here are some of our reasons:
The paralysis of Maddie de Garay was not reported in the Pfizer 12-15 year old clinical trial, and the FDA failed to investigate this case even though they knew about it. This is serious misconduct happening and nobody is holding the FDA accountable.
Adverse events were difficult to impossible to report (and Facebook conveniently removed the evidence of people complaining about that)
At least one death that happened didn’t show up. Who knows how many more?
The cohorts were not representative of the population as a whole (they were much healthier, e.g., rate of heart attacks was 10X lower than the overall population rate)
Five times as many people were disqualified from the treatment arm (311) compared to the control arm (61) for protocol violations even though the trial was supposed to be double blind.
Read this article on the Pfizer consent form. The consent form allows for participants who need emergency care and go straight to their doctor or hospital to be ejected from the study. But that’s hardly the only problem.
Pfizer paid one of the largest criminal fines ever imposed on a drug company for the arthritis drug Bextra.
The company can’t seem to find any safety signals even though it is obvious in VAERS.
No autopsies were done to determine the cause of death were done in the treatment group. This was a very serious oversight in our opinion. Nobody on the FDA or ACIP panel seemed to think this was a problem.
The death rates make no sense. We know of a 132 bed nursing home that had 2 deaths within hours of getting the vaccine. And a larger nursing home in Hawaii with over 500 beds had 32 deaths after vaccination. The numbers don’t match each other, but they are nowhere close to what was reported in the clinical trials which again suggests the cohorts were not representative of the population or that the company didn’t find the deaths or both.
THE LACK OF AUTOPSIES IS INEXPLICABLE
Autopsies are the gold standard for determining causality. But for these vaccines, it’s very tricky; you have to have the right skills and the right tests to make a proper diagnosis. Most medical examiners lack both.
How can the CDC say confidently that there have only been a few deaths? May we see the 249 autopsies? If not, why not?
In Germany, soon after the vaccines rolled out and deaths after vaccination started happening, the Federal Association of German Pathologists called upon the German authorities to require autopsies to validate the cause. Their requests were ignored presumably because nobody wants to know the answer.
In America, few people are asking for autopsies. And when they do, they are being denied
If we had the autopsies available, we wouldn’t have to debate whether we are right or wrong about the numbers of deaths -- we’d have the data.
The Norwegian Medicines Agency linked 13 deaths to vaccine side effects. At the time that article was published, there were only 13 assessments completed. So in 100% of the cases, the deaths were deemed to be caused by the vaccine by the official government agency.
In Germany, they actually did autopsies of 40 people who died within 2 weeks after vaccination. They determined that at least 30% to 40% died from the vaccine. From Media Blackout: Renowned German Pathologist's Vaccine Autopsy Data is Shocking... and Being Censored:
Dr. Peter Schirmacher is not just an average pathologist. The German doctor is world-renowned in his field, honored by The Pathologist as one of the 100 most influential in the world. He is the acting chairman of the German Society of Pathology, director of the Institute of Pathology at Heidelberg University Hospital, and president of the German Association for the Study of the Liver. Bottom line, this professor and doctor understands pathology like very few on the planet.
It is puzzling to us that nobody on the ACIP committee is calling for mandatory autopsies. Only 249 have been done on the 11,000 people who have died. It would be nice to know what they said.
It costs a family around $25,000 to $35,000 to do an autopsy that can take 90 days. But if the family calls it a COVID death, they can be paid $9,000 from FEMA. Are we surprised there are so many COVID deaths and so few autopsies?
Does ACIP think we should not have autopsies? I think it is important to clarify the committee’s opinion on whether we should have the data on why people are dying after the vaccine or whether ACIP would rather have coroners look the other way.
Right now, it seems to be difficult to have an autopsy done, so if you want to gather the data, I think it is important to say something rather than remain silent on this issue.
IT IS BECOMING CLEAR THAT THE VACCINES ARE RAPIDLY BECOMING LESS EFFECTIVE
As far as effectiveness, we believe the recent paper from a team of Japanese researchers, “The SARS-CoV-2 Delta variant is poised to acquire complete resistance to wild-type spike vaccines” shows that the vaccines we received will soon become completely useless to protect us and, to make matters worse, are already enhancing the ability of current variants to infect us through vaccine enhanced infection and/or replication (rather than “classical ADE” which so far appears not to be happening).
From the abstract:
Although Pfizer-BioNTech BNT162b2-immune sera neutralized the Delta variant, when four common mutations were introduced into the receptor binding domain (RBD) of the Delta variant (Delta 4+), some BNT162b2-immune sera lost neutralizing activity and enhanced the infectivity.
In short, even if the vaccine were perfectly safe and killed no one, vaccinating with a non-sterilizing vaccine in the middle of a pandemic is going to have a net negative benefit, exactly as Geert Vanden Bossche has been trying to tell the world since shortly after the vaccination program began. He called it a very serious mistake. Nobody in power listened.
The latest UK government data (Briefing #20), shows you are 57% more likely to die if you get delta and you are vaccinated than if you are unvaccinated. The computation for age<50 and fully vaxed vs. unvaxed is 13/48*147612/25536=1.57 which is consistent with the Japanese paper.
Therefore, not only are the vaccines not safe, but they are quickly becoming useless and may shortly be a liability as far as effectiveness is concerned.
EARLY TREATMENTS HAVE ALWAYS BEEN THE SAFER, MORE EFFECTIVE OPTION
Meanwhile, early treatments have been virtually ignored by mainstream academia and the NIH. Lack of suitable guidance from the NIH has caused the entire world to avoid early treatments. These treatments are both extremely safe and very effective. They work against all variants as well. For example, the protocols used by George Fareed and Bryan Tyson against COVID continue to work well against COVID and with over 6,000 patients treated in an area with one of the highest CFRs in the country, it is very rare for a patient to be hospitalized for COVID in their clinic; it only happens if the patient presents late. They have more than a 99% relative risk reduction against all COVID variants if the patients get treated early. The NIH has expressed no interest in trying to replicate this success despite the tremendous lifesaving potential and negligible risk. They are more interested in waiting for a new, unproven drug from Merck for treatment.
EARLY TREATMENTS HAVE BEEN CENSORED. NOBODY IN MEDICINE SEEMS TO MIND.
One of the earliest pioneers of early treatment, George Fareed, is banned for life from YouTube for trying to spread life-saving treatment protocols that work..
The Nobel Prize winning inventor of ivermectin, Dr. Satoshi Omura, had his video on ivermectin for COVID blocked on YouTube.
Ivermectin has several systematic reviews and meta-analyses showing that it works; the highest level of evidence in evidence-based medicine. But since this competes with the vaccine, everyone is instructed to ignore evidence-based medicine and replace it with the lowest level of evidence: expert opinion (e.g., from an agency).
In short, no matter what level of evidence you pass, it is not enough if it goes against the political false narrative.
We find it troubling that so few in the medical community are speaking out about such abuses.
These individuals are giving life-saving advice and have been censored and there are dozens of examples of many others that have been censored, banned for life, and/or demonetized.
It would be interesting to hear the ACIP members speak out on this subject, either endorsing the censorship or condemning it. Remaining silent on such an important issue will not help advance science and save lives. Normally, ACIP shouldn’t have to do this, but everyone else is remaining silent.
THE UK SAID THE VACCINE IS NOT RECOMMENDED FOR THOSE < 18 YEARS OLD
The UK panel said the data doesn’t justify vaccination of those under 18
Jul 19: UK opts not to vaccinate most under 18 against COVID-19
Then they changed their minds just 2 weeks later:
Aug 4: UK to roll out COVID-19 vaccines to 16 and 17-year-olds
Did the science really change that quickly? What new things were learned? Or is science being driven by politics which would be a new low point. If there was new science, it would be useful for everyone to know what it was.
16% NEVER CAME BACK FOR A SECOND SHOT. WHY?
62% of Americans are vaccinated vs. 52% who are fully vaccinated. So that’s 16% (52/62=.84) that never came back for a second shot
Why is there such a large gap when in order to do anything (like keep your job, go to school, etc) you need to be fully vaccinated?
We understand why people don’t get vaccinated at all (they are well informed). But what’s the reason for the 16% gap?
We know from user surveys that 3% of people who took the vaccine required treatment by a doctor. And 5% are still suffering from side effects. So that explains half of the gap. Basically 8% of people who got the vaccine had a large enough bad first experience, they aren’t going back for a second shot. This leaves 8% unexplained, but likely due to a bad first reaction.
We think that 12M injured Americans is a lot of people especially in light of the lack of an all cause mortality benefit and a clear lack of all-cause morbidity benefit. That’s a lot of people who have been injured for no proven net benefit (yes, COVID lives were saved, but it was an overall cost of lives). But that’s just our opinion.
SUMMARY
Analysis of multiple researchers using different sources confirms that the current COVID vaccines are very dangerous and are significantly increasing all-cause morbidity. The vaccines can trigger a wide range of serious neurological and cardiovascular symptoms, re-activate latent viruses, trigger flare-ups in people with cancer, and more. Multiple studies show 60% of patients have elevated D-dimers that persist for 3 months after vaccination.
These vaccines should be immediately halted. If they cannot be halted, then it is imperative that we inform the American public of the risks. Children, pregnant women, and previously infected people should be instructed to avoid vaccination. All vaccine mandates should end immediately until there is scientific proof of an all-cause morbidity and mortality benefit.
The censorship and intimidation of experts with dissenting opinions must end. You cannot speak the truth anymore on any social media platform without being blocked, banned, and/or demonetized. Pharmacies are allowed to not fill prescriptions on drugs and dosages that are proven to work in dozens of clinical trials: they can make these decisions without scientific evidence in support of their positions. They are not held accountable for their decisions.
Early treatment has always been a superior strategy for treating COVID: it is safer, more effective, and has a number of other important benefits. But it is being deliberately suppressed despite passing normal scientific milestones including large, well done Phase 3 trials and systematic reviews. Trials of ivermectin are being done by NIH that deliberately underdose the drug in order to prove to the world that it doesn’t work.
Virtually none of the people diagnosed with COVID in the hospital today were treated early with a “proven in clinical practice” early treatment protocol. That is the message we should be sending to America.
VOTE OF THE ACIP COMMITTEE WAS 14-0 IN FAVOR OF APPROVAL
They said they are there to protect the health of the public.
As far as we can tell, no member of the ACIP committee read this note or any of the other public comments submitted prior to the vote. So this comment didn’t matter. The public comments portal is just to placate the public.
There was no mention of early treatment as an alternative to vaccination.
This suggests to us that the committee is not interested in hearing from qualified people who disagree.
The data they presented was just one side of the story.
I loved how the slides showing bad data were left on the screen for like 2 seconds. And when the rate of severe adverse events was 10% vs. 2% for placebo, they just didn’t discuss that at all!
My favorite was Dr. Grace Lee’s presentation (VaST). Look at slide 18 which is from Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting (published in NEJM). It showed that the vaccines reduce your risk for pulmonary embolisms (PE) and intracranial hemorrhage (IH) compared to baseline pretreatment (the dotted line). Which is very interesting because our VAERS analysis (and the mechanism of action of the vaccine) showed the PE rates were off the charts. Anyone with a basic understanding of the mechanism of action of the vaccine and basic medicine would say there is no way PE can be reduced. However, nobody on the committee flagged this.
But PE risk is very very important. But our chart showed PE rates were elevated by 473 times. It was the most extreme event we saw in VAERS that was elevated.
To validate our results, the CDC itself found that two of the 14 kids (12-17 year old) died from PE and two from intracranial hemorrhage. What? According to the figure Dr. Lee presented, those two SAEs are both reduced by the vax. Yet based on our analysis, PE is 473X and IH is 42X more likely than baseline.
So this is a stunning divergence of reality vs. data presented to ACIP. And the death data is consistent with our VAERS analysis of SAE rates, and is not consistent with the clinical trial findings and the NEJM paper.
This is an objective example of how the data that they used to make the recommendation diverges from VAERS and nobody was interested in resolving the inconsistency. We got it right, but our data was never shown since it isn’t published.
From OpenVAERS search, we got 5164 PE events so 1411 events per million with 41X underreporting. The normal rate of PE is 0.39 per million. So this is an elevation of 3,617X from normal if we compare with the baseline incidence rate.
The science says only one hypothesis fits the facts: the vax is safe or it isn’t.
Here’s a table pulmonary embolism to help you decide which hypothesis is a better fit to the facts:
The point is that if you look for the hypothesis that is consistent with what is measured and observed, there is only one hypothesis that fits the data. That’s how science is supposed to work.
Today, science is about dropping critical thinking on the floor, censoring or ignoring qualified experts who disagree, and finding ways to support the mainstream political narrative. It is fitting the data to match the politics.
If ivermectin has a systematic review and meta-analysis published in a peer-reviewed journal, the NIH simply ignores the recommendation and pharmacies refuse to fill prescriptions. If NAC has caused no harm over 60 years, the FDA pulls it from the shelves and makes it prescription only while at the same time taking a vaccine which has killed over 200,000 people and making it available without a prescription and without warnings of just how deadly and/or disabling it is.
It’s very sad how quickly the wheels have come off the science bus.
OUR TEAM OF EXPERTS
Dr. Robert Malone, widely recognized as the inventor of the mRNA vaccine. He immediately recognized the dangers of the current vaccines when the biodistribution data was revealed after a FOIA request. He was one of the first people to go on record warning the world about vaccine enhanced infection and replication.
Dr. Geert Vanden Bossche, one of the few virologists in the world to warn the world about vaccinating with a non-sterilizing vaccine against a virus capable of mutation in the middle of a pandemic.
Dr. Byram Bridle, a highly respected viral immunologist at University of Guelph, did the FOIA request that exposed the biodistribution data showing the vaccines do not stay at the injection site like people thought, but instead cause the production of a toxin in all parts of the body including the brain.
Dr. Peter McCullough, Professor of Medicine, is the author of over 1,000 peer reviewed publications, He serves as editor of two journals and sits on the editorial boards of multiple specialty journals.
Dr. Ryan Cole, one of the few pathologists who has been unafraid to speak out.
Dr. Bret Weinstein host of the DarkHorse podcast, expert in evolutionary biology.
Dr. Chris Martenson, pathologist and host of Peak Prosperity on YouTube. Chris’s videos on YouTube are the most insightful videos about the virus and the vaccines.
Dr. Pierre Kory is our ivermectin expert, and one of our experts on early treatment.
Dr. Paul Alexander has expertise in the teaching of epidemiology (clinical epidemiology), evidence-based medicine, and research methodology. He is a former professor at McMaster University in evidence-based medicine; former COVID pandemic advisor to WHO-PAHO in Washington, D.C. (2020); and a former senior advisor on COVID pandemic policy at the U.S. government’s Department of Health and Human Services (HHS) in Washington, D.C.
Dr. Ira Bernstein, a physician in Canada. Bernstein replicated Hoffe’s D-dimer test which is extremely frightening.
Dr. Jessica Rose is an expert on the VAERS system. Her YouTube video on VAERS have never been challenged. She has a published paper on VAERS with several more on the way.
Dr. Meryl Nass, is a physician and VAERS expert.
Dr. Sin Hang Lee, an expert on DNA sequencing.
Mathew Crawford, is a mathematician and statistician who writes frequently about the pandemic including two articles on a serious CDC math error that no other person had noticed (Part I and Part II)
Dr. Charles Hoffe, is a physician in Canada.
Marc Girardot, is a member of PANDA. https://www.pandata.org/team/. PANDA is a politically and economically independent organization, focused on science-based explanations and tests them against international data. Marc has published extensively on the pandemic.
Dr. George Fareed, a physician in southern California who developed an extremely effective protocol for treating COVID-19 infections with a 99.76% risk reduction which is far more effective and safer than any vaccine
Tyson Gabriel is our mask expert. He produced this 1 hour instructional video. Nobody wants to challenge him to a debate on mask wearing.
Stephanie Seneff, senior research scientist at MIT. Although her field is computer science, she has an amazing breadth of knowledge in biology.
Aditi Bhargava, Professor, ObGyn and CRS, UCSF.
FDA response
Dear Mr. Kirsch,
While your email was not directly addressed to FDA, we would like to note that we do not agree with the analysis put forth in your comment, as we believe the data from VAERS that you reference were not properly interpreted. This is due to the limitations of VAERS itself, as well as limitations regarding certain private patient information that is not available to individuals outside of the FDA and CDC, as we noted in our correspondence to you dated July 27, 2021.
FDA and CDC have multiple systems in place to monitor the safety of COVID-19 vaccines, including VAERS. We continue to find that the COVID-19 vaccines have a favorable benefit-risk profile, supporting their use under Emergency Use Authorization. Additionally, FDA’s approval last week of Comirnaty (COVID-19 Vaccine, mRNA) followed a determination that the vaccine is safe and effective in preventing COVID-19 in individuals 16 years of age and older.
Sincerely,
Lorrie H. McNeill
Director
Office of Communication, Outreach and Development
Note to readers
The FDA response is what is known as hand-waving: they failed to point out a specific problem in our analyses and they failed to provide their own analysis showing the correct answer.
In short, they can’t dispute our arguments and have nothing in the tank on their end.
My response to the FDA
Lorrie,
Thanks. As promised, I will include your response in my comment so people can see your point of view.
It appears you did not read the material carefully. As we pointed out, the VAERS estimate we did was CONFIRMED with several other methods from independent researchers who used data outside the US and found the same numbers. Even with a $1M bug bounty, nobody found an error.
Since you didn’t like our analysis, perhaps you can show us YOUR analysis of the excess deaths in VAERS so we will show you the flaws in that analysis. We’d love to see your calculation of the “correct” propensity to report, the under-reporting factor used, and the subtraction of the background deaths.
Just today, I was talking with a physician, and he said he’s made one adverse event report in the last 29 years. This year alone, he’s made 25. I asked him why and he said, “well I’ve only ever seen one thing in the past 29 years that I’ve needed to report.”
I talked to a top neurologist who gave up on VAERS after filing 2 reports. She had 2,000 patients she wanted to report on. So that’s an under-reporting rate of 1,000X, and all of these 2,000 were serious.
And 2 days ago, I heard about a nursing home with 136 beds. They all got boosters. 4 died, 7 hospitalized. So we *could* be killing 4 people to save 1 person a year from COVID.
The point is this: ALL the evidence *we* have access to disagrees with the evidence *you* have access to.
One of us is right, one of us is wrong.
Can we meet with anyone at FDA so we can resolve the conflict?
This is important to resolve for the public. Peter Doshi and Daniel O’Connor will be happy to cover this so we can inform the public as well of the result of our discussions.
-steve
Attachments referenced
Estimating the number of COVID vaccine deaths in America (Attachment 2)
This document uses VAERS to estimate the total number of excess deaths caused by the vaccines. This estimate is validated using multiple other methods.
There is also a table of elevated adverse events showing the pulmonary embolism is elevated by 473 times above baseline (typical VAERS year).
Adverse Events Reported Following COVID-19 Vaccinations (Attachment 3)
This research by Professor Josh Guetzkow is an independent confirmation of two of the factors we found in our analysis:
VAERS isn’t being “over reported” this year as the FDA and CDC have falsely claimed due to greater “awareness” and propensity to report
VAERS isn’t be over-reported this year due to the number of vaccinations
To learn more about vaccine safety
Why so many Americans are refusing to get vaccinated
Is the latest article (250 pages long) and it has pointers to two 200 page articles with even more information. If you just read this article, you’ll be armed to answer any question that anyone will throw at you.
To learn more about early treatments and treating post-vaccine injury
Dr Bryan Ardis - Hospital Protocol Is What Is Murdering "Covid" Flu Patients
Dr Peter Doshi and Daniel O’Connor will be happy to cover this so we can inform the public as well of the result of our discussions.








